
There have been 34 laboratory-confirmed cases of monkeypox reported in Scotland since 23 May 2022. This includes an additional two cases since our last report on 28 June 2022. (PHS 1st July 2023).
Close contacts of the cases are being identified and provided with health information, advice and, where appropriate, vaccination.
Plans for a wider pre-exposure vaccination programme are in development for some healthcare workers who work in high-risk settings and some gay and bisexual men at higher risk of exposure. Full details on how eligible people can get vaccinated will be set out by Scottish Government in due course.
As of Thursday 30 June, there are 1,235 confirmed cases in the UK.
Wendi Shepherd, monkeypox incident director at UKHSA, said:
“The monkeypox outbreak continues to grow. Our investigations and information from confirmed cases continue to show that the overwhelming majority of cases are in gay, bisexual or other men who have sex with men.”
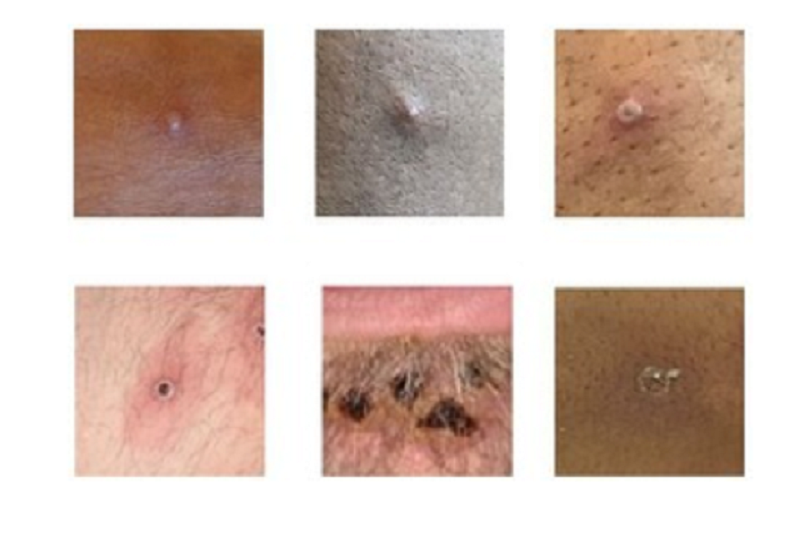
Anyone can get monkeypox and it can spread from person to person through:
- touching clothing, bedding or towels used by someone with the monkeypox rash
- touching monkeypox skin blisters or scabs (including during sex)
- the coughs or sneezes of a person with the monkeypox rash
| UK nation | Confirmed cases | Change since last report (26 June 2022) |
|---|---|---|
| England | 1,185 | +150 |
| Northern Ireland | 6 | +1 |
| Scotland | 34 | +7 |
| Wales | 10 | +1 |
| Total | 1,235 | +159 |
A high proportion of England cases were known to be London residents (77%, 692 of 898 with reported home address)
Information on the symptoms of and treatment for monkeypox are available on NHS inform.



Leave a Reply