
Published by Public Health Scotland on 13th April 2023 is the weekly national respiratory and Covid-19 surveillance report.
COVID
Changes in PCR testing guidance has reduced the numbers of tests available for sequencing compared to earlier in the pandemic.
The Office for National Statistics (ONS) published their final COVID-19 Infection Survey report on 24 March 2023. Therefore, COVID-19 surveillance will use a range of indicators including wastewater concentration levels, reported COVID-19 cases (PCR/LFD) and hospital activity.
Waster water Analysis – The last test in Orkney (Kirkwall) was published on 10th March 2023.
The purpose of COVID-19 testing has now shifted from population-wide testing to reduce transmission, to targeted, symptomatic testing in clinical care settings which has led to a reduction in the quantity and quality of available testing data. This makes it difficult to draw any conclusions from these data on community prevalence and caution is therefore advised when making comparisons between metrics and comparing trends over time. In the week ending 09 April 2023, there were 1,629 reported positive COVID-19 cases (compared to 2,149 in week ending 02 April 2023)
In the latest week ending 09 April 2023, there were 371 new COVID-19 admissions to hospital. Hospital admissions for the most recent week are provisional and should be treated with caution. At the time of publication there were no data available for one NHS Health Board, and the previous week’s figures have been rolled forward.

There were 34 COVID-19 admissions (3.4%) per 1,000 emergency admissions. In the same week, the 75-79 age group had the highest rate of COVID-19 admissions (5.8%) and the 18- 29 age group had the lowest rate (1.3%).
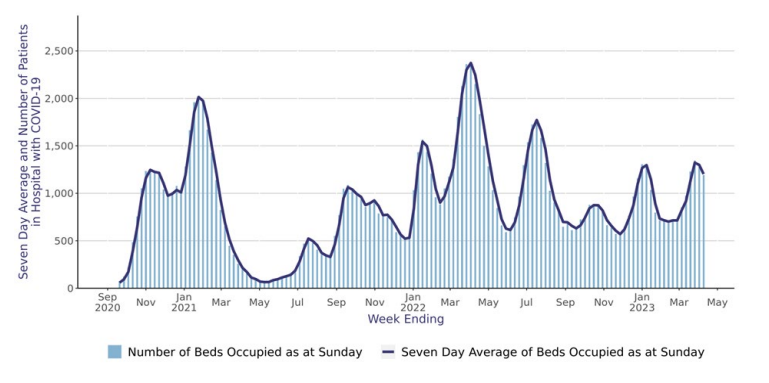
The number of COVID-19 patients in hospital is an indicative measure of the pressure on hospitals, as these patients still require isolation from other patients for infection control purposes.
There were 1,203 patients in hospital with COVID-19 which is a 7.4% decrease from the previous week ending 02 April 2023, when on average there were 1,299 patients.

There were 19 new admissions to ICU, an increase of 7 from the previous week (02 April 2023) when there were 12 admissions. There were on average 212 patients in ICU, of which 9.4% (20 patients) had a positive SARS-CoV-2 result.

The COVID-19 pandemic has direct impacts on health as a result of illness, hospitalisations and deaths due to COVID-19. However, the pandemic also has wider impacts on health, healthcare, and health inequalities.
VACCINATION
COVID-19 is a highly infectious respiratory infection.
This spring, COVID-19 booster vaccinations will be offered to those who are eligible:
- residents in care homes for older adults
- adults aged 75 years and over (or will turn 75 by 30 June 2023)
- people aged 5 years and over with a weakened immune system
Learn more about this year’s spring vaccination programme on NHS inform (external website).
Globally, as of 10:11am CEST, 12 April 2023, there have been 762,791,152 confirmed cases of COVID-19, including 6,897,025 deaths, reported to WHO. As of 11 April 2023, a total of 13,340,275,493 vaccine doses have been administered. (World Health Organisation)
Globally, 3 million new cases and over 23 000 deaths were reported in the last 28 days (13 March to 9 April 2023), a decrease of 28% and 30%, respectively, compared to the previous 28 days (13 February to 12 March 2023).
Contrary to the overall trend, important increases in reported cases and deaths were seen in the South-East Asia and Eastern Mediterranean regions and in several individual countries elsewhere. As of 9 April 2023, over 762 million confirmed cases and over 6.8 million deaths have been reported globally.



Leave a Reply